 Healthy ideas for your inbox
Healthy ideas for your inbox

In June 2020, Tina Allsop, an assistant principal at an elementary school in Bellingham, Washington, was busy adjusting to the many changes brought on by the COVID-19 pandemic. While working to implement Zoom practices and re-imagine what a school day looked like in a remote environment, she started experiencing frequent headaches and worsening vision.
Tina assumed these symptoms were caused by spending so much time looking at screens in her new virtual world.
“I spent eight hours a day on Zoom staring at a computer, so I attributed a lot of what was happening to me at the time to the COVID experience,” Allsop says. “I started getting headaches, and they were just kind of low-grade persistent headaches, but again, I was on the computer all day staring at a screen, and I just thought that’s what it was coming from.”
By January 2021, after several visits to optometrists and new eye prescriptions, one eye doctor noticed an abnormality in Allsop’s optic nerve and referred her to a specialist. The specialist recommended an MRI scan to examine the abnormality more closely and found a meningioma.
Meningioma: a common type of brain tumor
Meningiomas are tumors that arise from the tissues that envelop the brain and spinal cord called the meninges, and are the most common type of brain tumor. There are three different grades of meningiomas: Grade one, the most common, are slow-growing tumors; grade two, mid-grade tumors, have a higher chance of growing back after they’ve been removed; and grade three, malignant or cancerous tumors, are fast-growing.
Cancer is often random, but there are some factors that can increase the risk of developing a meningioma. These include being over age 65, being a woman, your genetics or previous brain radiation treatments. Other symptoms include loss of hearing or smell, migraine, tension headache, eye strain, sinusitis, confusion and seizures.
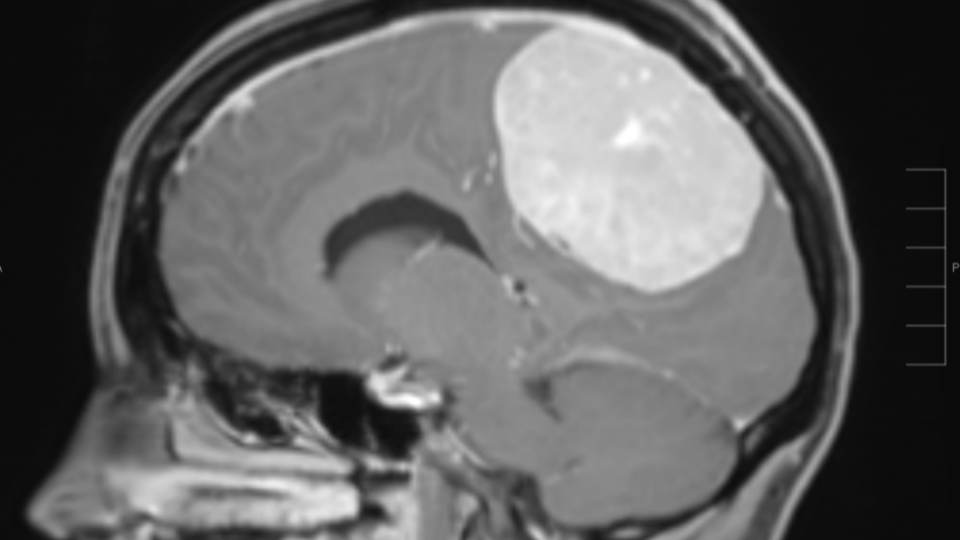
Allsop’s changes in vision and headaches were both potential symptoms of a meningioma. After the MRI, she was diagnosed with a very large, grade two meningioma.
“Tina had a tumor that was the size of a grapefruit and was actually invading the main draining vein from the brain called the superior sagittal sinus,” says Dr. Manuel Ferreira, UW Medicine’s chief of neurological surgery and co-director of skull base and minimally invasive neurosurgery. It was imperative to get the tumor out as soon as possible.
A successful surgery
About half of the 400 operations Ferreira does each year are for meningiomas, making him the perfect person to take on the case. Because of his experience, Ferreira was able to remove Tina’s entire meningioma and share the good news with her family.
“It was eye-opening to hear the head of neurosurgery for UW Medicine say, ‘I’m going to move mountains for you because this has to happen immediately — it’s serious,’” says Ryan Allsup, Tina’s husband.
Ferreira says that with the tumor removed, the need for lifelong tumor control, with radiation or chemotherapy, is very low.
Two months into her surgery recovery, with the help of physical therapy, Tina could walk independently. About three months after the surgery, she could do a slow hike up the trail near her house. Four months later, she gradually started getting back to normal.
“Being able to hike again was one of my number one goals,” Tina says. “Another one of my goals was that summer to be back on a paddleboard out at the lake. And so, Ryan got me a paddleboard for my birthday, and by June, I was shaky, but I was on it, and that was another big milestone.”
This experience acted as a teacher in many ways — the most important lesson being that paying attention to new or unusual symptoms in your body is crucial. Tina and her family’s persistence led to timely and effective treatment of her meningioma.






